

Overview of the Spine:
The spine is a critical structure in the human body, designed to bear weight and enable a wide range of movements. This is made possible by specialized structures known as spinal discs. There are 23 spinal discs (also referred to as intervertebral discs or spinal disks) in the human spine, starting from the disc between the axis (C2) and the third cervical vertebra (C3) to the one between the fifth lumbar vertebra (L5) and the sacral base (S1). Spinal discs collectively account for approximately 25% of the spine’s total length, progressively increasing in size from the neck to the lower back.
Functions of the Spine and Spinal Discs
Spinal discs are remarkable, highly specialized structures that play essential roles in the body’s movement and stability. A healthy spinal disc is vital for maintaining an active and discomfort-free lifestyle. Below are the primary functions of the spine and spinal discs:
- Protection
- Spinal Cord and Nerve Roots: Protects the delicate nervous tissue responsible for communication between the brain and body.
- Internal Organs: Safeguards many vital organs within the torso.
- Points for Attachment
- Provides anchor points for ligaments, tendons, and muscles essential for movement and stability.
- Structural Care
- Care the head, shoulders, and chest.
- Connects the upper and lower body while balancing and distributing body weight.
- Flexibility and Mobility
- Enables various movements such as flexion (forward bending), extension (backward bending), side bending, and rotation.
- Allows for combinations of these movements for complex actions.
- Other Functions
- Bone Marrow: Produces red blood cells within the vertebrae.
- Mineral Storage: Acts as a reserve for essential minerals like calcium and phosphorus.
Regular assessments and targeted care are vital to maintaining a healthy spine and spinal discs, as they directly influence overall health and mobility.
Regions of the Spine
The spinal column (also known as the vertebral column) extends from the skull to the pelvis. It comprises 24 movable bones, the sacrum, and the coccyx. The vertebrae stack on top of each other to form the spine. There are three primary regions of the spine:
- Cervical Spine (Neck)
- Thoracic Spine (Mid-Back)
- Lumbar Spine (Lower Back)
Additionally, the sacrum and coccyx are non-movable regions that collectively contribute to the vertebral column. Let’s take a closer look at each region:
Cervical Spine
The cervical spine consists of seven vertebrae (C1–C7) and is divided into two parts:
- Upper Cervical Region: Includes the Atlas (C1) and Axis (C2).
- Lower Cervical Region: Comprises vertebrae from C3 to C7.
The Atlas (C1 Vertebra): The Atlas maintained the skull and is named after the mythological figure who held up the world. It is a ring-like structure with two lateral masses joined by anterior (front) and posterior (back) arches.
The Axis (C2 Vertebra): The Axis is named for its role in the rotation of the head and neck. Located directly below the Atlas, the Axis acts as the pivot point for the head. It is the strongest and thickest of all cervical vertebrae.
Thoracic Spine
The thoracic spine consists of 12 vertebrae (T1–T12) that increase in size from top to bottom. Key features include:
- Small Pedicles: Provide structural care.
- Long Spinous Processes: Offer stability but limit mobility.
- Intervertebral Foramina: These neural passageways reduce the likelihood of nerve compression.
The thoracic spine connects posteriorly to the rib cage and anteriorly to the sternum. Floating ribs are found at T11 and T12, as they do not attach to the sternum. The thoracic spine’s mobility is restricted due to its rib connections and the elongated spinous processes.
Lumbar Spine
The lumbar spine includes five vertebrae (L1–L5) and bears the majority of the body’s weight. This region is prone to biomechanical stress and injuries.
Key Features of the Lumbar Spine:
- Pedicles: Longer and wider than in the thoracic spine, providing robust care.
- Spinous Processes: Horizontal and square-shaped, aiding stability.
- Intervertebral Foramina: Large openings but with the highest risk of nerve compression due to increased mobility and load-bearing demands.
The lumbar spine’s structure ensures it maintains both movement and weight efficiently while being highly susceptible to strain and injury from improper biomechanics.
The Vertebrae

The vertebrae are the individual bones that make up the spine, specifically designed to bear weight in a bipedal posture. Unlike other species, human vertebrae are uniquely adapted for this function, with characteristics that facilitate both movement and stability.
Key Facts About Vertebrae:
- The vertebrae form a column from just below the skull to the tailbone.
- There are 24 vertebrae in total, excluding the tailbone.
- Technological advancements like MRI have significantly improved our understanding of the vertebrae and their role in spinal health.
Understanding the intricate relationship between the spinal column and its discs is essential for maintaining a healthy, active lifestyle. Spinal health is foundational to overall well-being, making regular check-ups and targeted interventions critical for preserving mobility and quality of life.
The Vertebral Body
Structure and Role: The vertebral body is the largest and most prominent part of each vertebra. It is primarily cylindrical in shape and varies in size, being smallest in the neck region and largest in the lower back. The Atlas (the first cervical vertebra) is unique in that it lacks a vertebral body. In total, there are 23 vertebral bodies in the human spine, as the first vertebra does not have one.
At the top and bottom of each vertebral body lies a cartilaginous structure known as the vertebral end-plate (or epiphyseal plate). These end-plates are securely attached to the vertebral body and serve as critical points of connection to the spinal discs.
Functions:
- Weight-Bearing: The vertebral body bears the bulk of the spine’s weight.
- Structural Care: It serves as the anterior (front) portion of the vertebra, from which the vertebral and neural arches originate.
- Spinal Protection: The neural arch forms a protective boundary around the spinal canal, safeguarding the spinal cord and nerves.
The Vertebral End-Plates
Structure and Importance: Each vertebra has two vertebral end-plates, located on the top and bottom of its vertebral body. These end-plates are closely linked to the intervertebral discs and are considered integral to disc health.
Functions:
- Attachment: They anchor the intervertebral discs to the vertebral body.
- Nutrient Supply: The end-plates are the primary source of nutrients for the spinal discs.
- Stabilization: They contribute to maintaining the structural integrity of the spine.
The human spine contains 46 vertebral end-plates, which encapsulate the intervertebral discs above and below.
Spinal Disc Structure and Function
Spinal discs sit between each bone of the spine and help the spine move, bend, and handle daily load. Each spinal disc connects one level of the spine to the next while keeping movement controlled and stable.
Each spinal disc has a clear role. It helps absorb pressure, allows smooth motion, and spreads forces across the spine. It also works closely with nearby joints, ligaments, muscles, and end-plates so the neck and back function as one coordinated system.
There are 23 spinal discs in the human spine:
- 6 in the neck (cervical spine)
- 12 in the mid-back (thoracic spine)
- 5 in the lower back (lumbar spine)
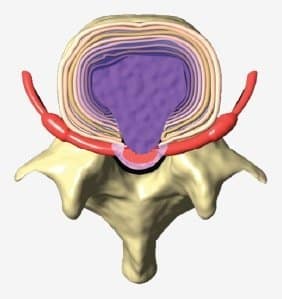
Each spinal disc is made of three main parts:
- Nucleus pulposus – a soft, gel-like center that helps distribute load
- Annulus fibrosus – a strong outer layer made of collagen fibers that contains and protects the inner core
- Vertebral end-plates – thin layers that connect the disc to the spinal bones and allow nutrient exchange
These parts work together to help the spinal disc manage pressure and movement throughout the day.
Spinal discs are made mainly of water, collagen, and proteoglycans. These components help maintain hydration, flexibility, and the ability to handle mechanical stress.
A healthy spinal disc adapts to everyday activities such as sitting, walking, bending, and lifting. Over time, changes in hydration and tissue quality may affect how the disc manages load. When that happens, nearby joints, ligaments, and spinal nerves may also be influenced.
Understanding how spinal discs are structured and how they function helps explain why they play a central role in how the spine performs day to day.
Vertebral Body Articulation
The vertebral body articulations are cartilaginous joints stabilized by three key components:
- The Anterior Longitudinal Ligament (ALL)
- The Posterior Longitudinal Ligament (PLL)
- The Intervertebral Discs (IVD)
The Anterior Longitudinal Ligament (ALL)
The ALL connects the vertebral bodies along the front of the spine. It runs from the axis (C2) to the sacral base (S1), attaching firmly to each intervertebral disc. This ligament serves as a protective barrier for the discs and provides structural care to the spine. It is narrow at the top (near the cervical spine) and widens as it descends to the lumbar region.
Functions of the ALL: The ALL plays a multifaceted role in spinal health and stability, including:
- Providing Stability: Limits excessive spinal extension and maintains the alignment of the vertebrae.
- Protecting the Spinal Discs: Acts as a barrier to minimize stress on the intervertebral discs.
- Connecting Vertebrae and Discs: Serves as an anchoring point between the vertebral bodies and the discs.
- Distributing Mechanical Forces: Helps evenly distribute forces applied to the spine during movement or weight-bearing activities.
Calcification of the ALL: Calcification of the ALL, often due to familial predisposition, unmanaged injuries, or wear and tear, can result in discomfort and limited range of motion.
This condition is similar to calcification of the Posterior Longitudinal Ligament (PLL), which impacts spinal mobility and stability.
Spinal Disc Care at CSC: CSC specializes in addressing the health of the spinal disc and its maintain structures. With targeted therapies and modern technology, we ensure that every aspect of your spine’s care system is optimized for recovery.
The Posterior Longitudinal Ligament (PLL)
The PLL attaches from the axis (C2) and runs along the posterior surface of the spinal column down to the first sacral segment (S1). Unlike the anterior longitudinal ligament, the PLL is broader at the top and narrows as it descends toward the lower back. It connects to both the spinal discs and a small portion of the vertebral body.
Key Characteristics of the PLL: The PLL is positioned along the anterior aspect of the neural canal.
- It attaches to the outer fibers of the spinal disc, ensuring stability.
- It lies close to the spinal dura mater, separated by loose areolar tissue, which houses the internal vertebral venous plexus.
- The rich nerve supply of the PLL includes discomfort-sensing nerve fibers that act as a defense mechanism. These fibers alert the body to harmful events, such as inflammation or compression from a bulging or herniated disc.
Functions of the PLL: Vertebra-to-Vertebra Connection: Maintains spinal stability by linking adjacent vertebrae.
- Disc-to-Vertebra Connection: Secures the spinal disc to the vertebral bodies above and below.
- Disc Stabilization: Strengthens the spinal discs, maintaining their load-bearing function.
- Spinal Cord Protection: Shields the spinal cord from compressive forces caused by discs or bone spurs.
Calcification of the PLL: njury or repeated trauma can lead to thickening or calcification of the PLL. This condition is often associated with unmanaged sports injuries, auto accidents, or chronic conditions such as cervical spondylosis. Calcification can result in discomfort, limited mobility, or even disability if left unaddressed.
Signs & Risks of PLL Calcification:
- Increased risk of neck stiffness or discomfort.
- Potential for nerve irritation or compression.
- Likely connection to conditions such as spinal canal narrowing or spondylosis.
Importance of Proper Evaluation & Care:
Unmanaged injuries or conditions involving the PLL can lead to progressive complications. If you have a history of sports injuries, auto accidents, or a diagnosis like cervical spondylosis, timely evaluation is essential to prevent further damage.
Our clinical teams are equipped with the expertise and technology to provide targeted care for PLL-related issues. If you or a loved one experiences persistent neck discomfort, consider visiting one of our centers for a thorough assessment and holistic care.
Share this information to raise awareness about the significance of spinal ligament health and its impact on the spinal cord and overall well-being. Early detection and care are key to preserving mobility and preventing long-term complications.

The spinal disc, also referred to as the vertebral disc, is a specialized structure located between the vertebrae of the spine. Acting as a cushion and stabilizer, spinal discs serve as shock absorbers, ligaments that bind the vertebrae, and pivotal points that allow movement. These discs are present at every vertebral segment except between the first and second cervical vertebrae.
There are 23 spinal discs in the human spine, beginning between the axis (C2) and the third cervical vertebra (C3), and ending between the fifth lumbar vertebra (L5) and the sacral base (S1). Together, they account for approximately 25% of the spine’s total length and gradually increase in size from the neck to the lower back. These discs also play a significant role in forming the spinal column’s secondary curves, with thickness variations depending on their location.

Spinal discs are reinforced by the anterior and posterior longitudinal ligaments, further enhancing their stability and resilience. Their ability to withstand pressure and absorb shock is critical for protecting the spine and maintaining overall bodily function.
The Structure of a Healthy Spinal Disc
A healthy adult spinal disc is the largest avascular structure in the human body, relying on diffusion for nutrition. Its composition includes three main components:
- Vertebral End-Plates
- Annulus Fibrosus
- Nucleus Pulposus
Although their structural roles differ, the spinal disc’s three components rely on:
- Proteoglycan (protein-based molecules for water retention)
- Collagen (cartilage for strength and flexibility)
- Water (constituting up to 80% of the disc’s volume in a healthy state)
The Annulus Fibrosus

The annulus fibrosus is the disc’s sturdy outer layer, composed of type 1 collagen fibers. These fibers are critical for containing the highly pressurized nucleus pulposus. Additionally, the annulus attaches to the vertebral end-plates, further anchoring the disc to the spinal bones.
Characteristics of the Annulus Fibrosus:
- Composition: The outer layer is made of fibrous tissue, while inner layers consist of cartilage-like sheets known as lamellae.
- Strengthening Mechanism: Approximately 15 to 25 concentric layers of lamellae are arranged in an ‘X’-like configuration at 45-degree angles, enhancing the annulus’ ability to resist pressure and maintain stability.
- Innervation: The outer layer is innervated by the Sinuvertebral Nerve, a mixed nerve containing both sensory and sympathetic fibers. This is why damage or stress to the annulus can cause discogenic discomfort, a sharp and localized discomfort originating from the disc.
The Importance of Annulus Fibrosus
The Annulus Fibrosus, the outermost layer of the spinal disc, is a critical component for spinal health and function. Unlike the inner layers and nucleus, the very outer layer of the annulus is vascular, meaning it has a blood supply. The middle and inner layers, along with the nucleus pulposus, are entirely avascular, depending on diffusion from surrounding structures for nutrients.
Tiny capillary beds embedded in the subchondral bone of the vertebral end-plates provide the nutrients needed for the avascular portions of the disc. This subchondral vascular network facilitates the diffusion of essential elements such as water, oxygen, glucose, and amino acids. Nutrients “soak” through the vertebral end-plates into the spinal disc, caring its health and vitality.
The Nucleus Pulposus
The nucleus pulposus, located at the center of the disc, is responsible for shock absorption and load distribution. Comprised primarily of proteoglycan, it has a remarkable ability to retain water, with water content making up approximately 80% of its composition in a healthy state.
Functions of The Nucleus Pulposus:
The nucleus pulposus is the water-rich (80% water), gelatinous, and highly elastic central structure of the spinal disc. It is soft, pulpy, and highly pressurized, making it essential for spinal mobility and weight-bearing. The nucleus is proportionally larger in the cervical and lumbar spine due to the higher mobility demands in these regions. Its three primary functions are:
- Weight-Bearing: Maintain and distributes the body’s weight.
- Pivot Point: Serves as the central point of movement for spinal flexibility.
- Ligament Function: Binds adjacent vertebrae together, providing structural integrity.
How Do Spinal Discs Absorb Nutrients?
The diffusion process required to nourish the spinal disc depends on the movement and pressure changes in the spine. Gentle stretching and relaxation of a healthy spine encourage diffusion through a mechanism called imbibition.
Natural Imbibition & Diurnal Changes
One of the most natural forms of imbibition occurs through diurnal changes, as the body experiences periods of compression and decompression over a 24-hour cycle. During sleep, when the spine is unloaded, the spinal discs absorb fluids and nutrients, increasing in volume. This process can expand a healthy spinal disc by approximately 20%, adding up to 19mm in stature overnight. This natural height variation is why people are often slightly taller in the morning.
What Is Imbibition & Its Role in Spinal Disc Health?

Imbibition refers to the process by which spinal discs absorb nutrients and maintain hydration. It is crucial for the health and functionality of the Nucleus Pulposus, the disc’s central component made primarily of proteoglycan, a protein that attracts water.
How Imbibition Works:
When the spinal disc is compressed, moisture is forced out.
Upon relieving the compressive force, water and nutrients are drawn back into the disc through the end-plates.
This cyclical process ensures that the nucleus pulposus remains hydrated and nourished.
Imbibition is akin to how a sponge absorbs water: compression expels fluids, and decompression draws them back in. This mechanism is essential for a healthy spine, enabling the discs to sustain normal function and maintain their structural integrity.
The Importance of Imbibition for Preventing Disc Degeneration
Without proper imbibition, the nucleus pulposus and the entire disc can degenerate, leading to reduced functionality and potential spinal disorders. Activities and therapies that promote imbibition, such as non-invasive spinal decompression, are essential for maintaining disc health. Targeted spinal care and movement-based therapies encourage this natural process, helping prevent or reverse spinal disc degeneration.
Contact Chiropractic Specialty Center® for comprehensive care designed to optimize spinal health through therapies that enhance imbibition and disc regeneration.
Clinical Implications of Spinal Disc Disorders
Disruption or degeneration of spinal discs, particularly in the annulus fibrosus, can result in conditions such as:
- Discogenic discomfort (originating from the disc)
- Slipped discs (disc bulges, herniations, or prolapses)
- Osteophyte formation (bone spurs)
These conditions often require targeted care to address the root cause. Chiropractic Specialty Center® (CSC) offers modern non-surgical methods, such as NSD Therapy®, to repair and rejuvenate damaged discs.
Vertebral End-Plate
The vertebral end-plate is a thin cartilaginous structure capping the top and bottom of each vertebra from C2 to L5. Measuring approximately ¾ millimeter thick, the vertebral end-plates are not part of the vertebral bone but instead are interwoven into the disc’s annulus fibrosus. This integration makes them functionally part of the spinal disc.
Key Features:
Nutrient Supply: The spinal discs are avascular (lacking blood supply), so nutrients are diffused through the vertebral end-plate to the inner two-thirds of the annulus fibrosus and the entire nucleus pulposus.
Biochemical Makeup: The end-plates have a high concentration of water and proteoglycans at their center, while the periphery contains more collagen. This structure facilitates the diffusion of essential nutrients between the vertebrae and the disc.
How Spinal Discs Get Damaged
As the day progresses, axial loading (compression caused by body weight and activity) affects the spinal discs, much like squeezing a sponge. This compression expels water and nutrients from the disc, gradually increasing intradiscal pressure (pressure within the disc).
Key Processes During Axial Loading
Fluid Loss: Mild axial loading can lead to a 1.5mm reduction in disc height, correlating with a 12% fluid loss from the annulus fibrosus and a 5% fluid loss from the nucleus pulposus.
- Reduced Nutrient Infusion: Prolonged axial loading increases intradiscal pressure, potentially exceeding diastolic blood pressure and halting the infusion of nutrients and oxygen into the discal cells.
- Increased Intradiscal Pressure: Non-load-bearing pressure averages 70mm Hg, but excessive loading prevents proper diffusion of nutrients, leading to degradation.
Effects Of Prolonged Axial Loading (Creep Loading)
Creep loading refers to prolonged axial compression of the spine, which can cause significant damage over time.
- Dehydration of Disc Components: Both the annulus fibrosus and nucleus pulposus lose water content, diminishing their shock-absorbing ability.
- Loss of Nutrients: Reduced fluid exchange leads to poor nutrient delivery, compromising disc health.
- Proteoglycan Loss: The breakdown of proteoglycans, essential for water retention, results in degradation of the disc’s aggrecan molecules. The loss of proteoglycans is the most significant biochemical change linked to disc degeneration.
To maintain spinal disc health, minimizing prolonged axial loading and encouraging proper hydration and nutrient diffusion are critical. Chiropractic Specialty Center® offers modern non-surgical spinal disc care to mitigate damage and encourage regeneration through targeted therapies. Contact us today for comprehensive spine health solutions.
Proteoglycans and Spinal Disc Health

Proteoglycans are critical structural components of the spinal disc, forming the building blocks of the aggrecan molecules that maintain the disc’s hydration and elasticity. These molecules are synthesized by the chondrocyte-like cells in the nucleus pulposus and the inner annulus fibrosus. Proper nutrient flow to the disc is vital for the production of proteoglycans, which ensures the disc’s ability to withstand weight-bearing forces and maintain overall spinal health.
Impact of Proteoglycan Loss on Spinal Discs
When the flow of nutrients is disrupted, proteoglycan production diminishes, leading to significant changes in the spinal disc’s mechanical properties. Here are some critical effects of proteoglycan loss:
- Reduced Hydration: A decrease in osmotic pressure results in the disc’s inability to retain water under load, reducing its shock-absorbing capacity. Dehydrated discs lose height and fluids more rapidly, making them prone to bulging or herniation.
- Altered Load-Bearing Behavior: Without proper hydration, the spinal disc loses its hydrostatic properties. This shift increases stress on the vertebral end-plates and the annular fibers, leading to tears, bulging, or even herniation.
- Disc Degeneration and Height Loss: Loss of disc height alters the biomechanics of the spine, subjecting nearby structures, such as the facet joints, to abnormal loads. This process may result in osteoarthritis in these joints. Reduced tension on the ligamentum flavum can lead to thickening (hypertrophy), contributing to spinal stenosis.
Correlation Between Proteoglycan Loss and Degeneration
Medical research using MRI scans has demonstrated a strong correlation between disc degeneration and the depletion of proteoglycans. Degenerated discs no longer maintain their structure or function efficiently under pressure, setting the stage for additional damage. These effects can lead to:
- Ligamentum flavum thickening into the spinal canal.
- Tears in the annulus fibrosus, which weaken its structural integrity and allow the nucleus pulposus to migrate.
- The progression of spinal disc disorders such as bulging, prolapsed, or herniated discs (commonly referred to as a slipped disc).
The Mechanics of Disc Herniation
A healthy spinal disc is resilient and does not herniate under normal physiological conditions. Laboratory studies have shown that excessive mechanical forces far beyond everyday activities are required to rupture a healthy disc. In most cases, the vertebral body fails before the disc does. However, degenerative changes make the disc significantly more susceptible to herniation:
- Annular Tears: Prolonged axial loading, repetitive strain, or trauma can create microtears in the annular fibers, weakening the disc’s structure.
- Nucleus Pulposus Migration: These tears allow the nucleus to migrate toward the weakened areas, leading to disc bulging or herniation.
- Nerve Compression: Herniated discs commonly protrude posteriorly or posterolaterally, pressing on nerve roots in the spinal canal or foramina, causing numbness and tingling and other symptoms.
The loss of proteoglycans is the primary factor driving spinal disc degeneration. Prolonged stress, repetitive motion, and unmanaged microtrauma can accelerate these degenerative changes, leading to spinal disc disorders. Early intervention through targeted non-surgical care is essential to halt or reverse disc damage.
Comprehensive Spinal Decompression and Spinal Disc Damage

When pressure within the disc is lowered in a controlled manner, it may allow improved fluid exchange through the end-plates. This process is closely linked to disc hydration and the natural cycle of loading and unloading that occurs throughout the day.
In clinical settings, decompression-based approaches are often combined with movement-based physiotherapy, joint-focused chiropractic methods, and structured rehabilitation. These are typically selected based on individual findings, with the goal of improving how the spine moves, distributes load, and adapts over time.
Exercise and rehabilitation are commonly included as part of this process. These may focus on controlled movement, posture awareness, and gradual reconditioning to help the spine manage daily mechanical stress more effectively
The Role of Spinal Discs in Neck and Back Symptoms
The spine is made up of small bones called vertebrae, which are stacked to form the spinal column. Between each vertebra sits a spinal disc, a structure that helps absorb mechanical load and allows controlled movement.
Changes in disc structure, such as reduced hydration, bulging, or herniation, may influence nearby spinal nerves. When this occurs, symptoms may extend beyond the spine and be felt in other areas of the body.
These may include:
- Arm discomfort or tingling, often linked to changes in the cervical (neck) region
- Leg discomfort, tingling, or radiating sensations, commonly associated with sciatic nerve involvement
If you would like to better understand how nerve-related leg symptoms develop, you may also read our page on sciatica and nerve-related leg discomfort.
Non-invasive spine care focuses on helping the spine move and handle daily load more efficiently without the use of injections or surgery. These approaches look at how the spine functions as a whole rather than focusing on a single structure.
Care may include a combination of gentle chiropractic methods, physiotherapy, and structured rehabilitation. Each part plays a role in improving movement, muscle balance, joint coordination, and how forces are shared across the spine.
Some approaches also consider how spinal discs respond to changes in load and movement. This includes working with the body’s natural process of fluid exchange within the disc, using gradual and controlled input over time.
Understanding how non-invasive spine care is structured can make it easier to explore suitable options for spinal disc concerns, especially when the goal is to improve movement, function, and day-to-day comfort.
NSD Therapy® and Disc-Focused Non-Invasive Care
NSD Therapy® is a non-invasive, disc-focused care approach that looks at how spinal discs respond to changes in load, positioning, and movement. It is typically included as part of a broader plan that also considers joint function, muscle activity, and overall spinal coordination.
This approach focuses on applying controlled and gradual changes in spinal positioning. These changes may influence pressure within the disc and work alongside the body’s natural fluid exchange process through the vertebral end-plates. This process is important for maintaining disc hydration and normal disc function.
In practice, disc-focused care is often combined with gentle chiropractic methods, physiotherapy, and structured rehabilitation. These elements are used together to improve how the spine moves, distributes load, and adapts to daily activities.
Understanding how NSD Therapy® fits within a structured, non-invasive care approach can help when exploring options for spinal disc concerns, especially when considering how movement, load, and disc behavior are connected.
Understanding Traction Methods for Neck & Upper Spine Care

Mechanical traction has been used for many years as a way to apply a gentle pulling force to the spine. In the neck region, some systems use a harness that supports the chin and back of the head, as seen in the image above. This setup creates a lifting force through the jaw and upper neck.
While the intention is to create space between spinal segments, the way force is delivered matters.
Many traditional traction and DTS-style systems apply a straight-line pull, often in repeated pull-and-release cycles. These movements are not always specific to individual spinal levels. In some cases, the body may respond by tightening surrounding muscles, especially in sensitive areas like the neck and upper back. When that happens, the intended effect on spinal discs and joints may become less consistent.
The neck is a highly mobile and delicate region. It also connects directly to the upper back, where posture, muscle balance, and joint mechanics all play a role. Because of this, care approaches for the neck should consider more than just a simple pulling force.
A more structured approach focuses on:
- Controlled positioning of the spine
- Gradual, measured force application
- Attention to individual spinal segments
- Integration with movement, muscle work, and rehabilitation
These factors are especially important for individuals dealing with:
Understanding how traction is applied—and how the body responds—can help guide better decisions when exploring non-invasive spine and joint care options.